Read here what's moving us right now.WIKI-MEDIACC-Bereich an.

Ein persönlicher Meilenstein: Beitrag zur DIN EN ISO 14155:2026
Ich habe an der neuen DIN EN ISO 14155:2026 mitgewirkt!

Wird sich Endometriose bald an Biomarkern im Blut erkennen lassen?
Endometriose könnte schon bald früher erkannt werden, dank eines neuen Biomarkers.

Depression: Kann ein Parkinson-Medikament die Freude zurückbringen?
Ein zentrales Symptom der Depression ist die Anhedonie, das Unvermögen, Freude zu empfinden. Nun gibt eine neue Studie aus Schweden Grund zur Hoffnung.

RUPERT – Die digitale psychologische Anlaufstelle für unsere echten Helfer:innen!
Endlich gibt es ein Pilotprojekt zur psychologischen Unterstützung von Einsatzkräften: RUPERT.

Pädiatrische klinische Prüfungen in Europa: Noch immer steht die Sprachbarriere im Weg
Vor allem für Kinder ist Sprache ein großes Hindernis bei der Studienteilnahme.

Süße Getränke, bittere Folgen? Was Zucker in der Schwangerschaft anrichten kann
Regelmäßiger Konsum von Süßgetränken während der Schwangerschaft schadet dauerhaft dem Ungeborenen, stellt eine neue Studie aus Japan fest. Schuld ist vor allem Fruchtzucker.
Gesundheitstracking mit Wearables – Bringt es uns weiter?
Mit Smartwatch & Co. gesammelte Daten und Informationen werden genutzt, um das eigene Wohlbefinden zu optimieren, wenn man nicht auf sein Gefühl vertrauen möchte. Doch kann der Arzt oder die Ärztin damit etwas anfangen?
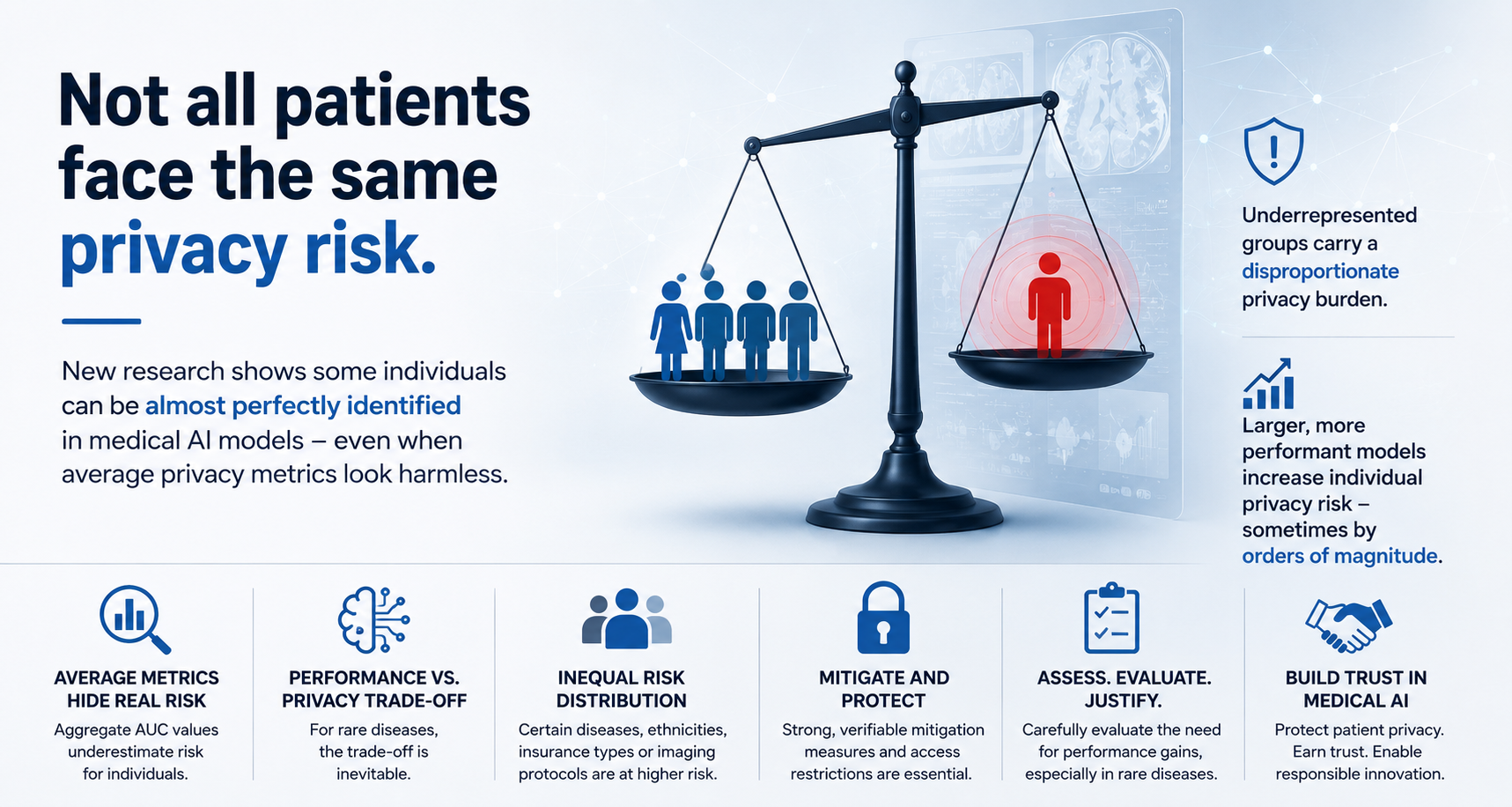
Ungleiche Datenschutzrisiken bei medizinischer KI: Was Hersteller jetzt angehen sollten
Patientendaten in der medizinischen KI sind nicht „nur“ ein datenschutzrechtliches Thema – sie stellen ein ungleichmäßig verteiltes Risiko dar.

Zu viele Worte für „Vereinfachung“? Was der SANT-Ausschuss des Europäischen Parlaments vorschlägt
Der jüngste Reformentwurf für die MDR und die IVDR kommt mit einem 79 Wörter langen Titel, sechs Themenbereichen und Verweisen auf vier verschiedene Verordnungen daher. Wo ist da die Vereinfachung?

Von smarten Sensoren zu smarten Behauptungen: Warum Beweise das fehlende Glied bei KI-Wearables sind
KI-Wearables generieren kontinuierlich große Datenmengen – oft von zertifizierten Medizinprodukten oder von Systemen, die sich in der Zulassungsphase befinden. Auf dem Papier sieht das beeindruckend aus. In Gesprächen mit Aufsichtsbehörden, Kostenträgern oder klinischen Partnern ist plötzlich eine Frage wichtiger als alle technischen Details: Was lassen diese Daten zuverlässig erkennen?
Demonstrate the medical benefits of your product
With our many years of experience and expertise, we offer effective solutions to demonstrate the medical benefits of your product.
From the conception to the execution of preclinical and clinical investigations, we support you with customized services.
Find out how MEDIACC can help you achieve reimbursability for your products.